I understand that my authorization will remain effective from the date of my signature until and that the information will be handled confidentially in compliance with all applicable federal laws. i understand that i may see the information that is to be sent, and that i may revoke the authorization at any time by written, dated communication. Sf 182 authorization, agreement, and certification of training revised 4/12/2021. sf 28 affidavit of individual surety renewed 3/24/2021. of 90 release of lien on real property cancelled 3/23/2021. gsa 3690 employee's service agreement for receipt of a retention incentive revised 3/18/2021. Medical release form pdf. fill out, securely sign, print or email your generic authorization to release medical information form instantly with signnow. the most .
Name of patient: date of birth: i. authorization for release of information and for redisclosure. i authorize. whose address . Hipaa compliant authorization for the release of patient information pursuant to 45 cfr 164. 508. i authorize and request the disclosure of all protected information for the purpose of review and evaluation in connection with a legal claim. i expressly request that the designated record custodian of all covered entities under hipaa identified.
Authorization letters to release information play a significant role in financial, legal, business, and civil matters. one must go through the sample letters to better understand the different ways to tailor the letters to fit the purpose. each authorization letter is normally different depending on the reason for granting permission. Authorization to release healthcare information. this authorization to release form template authorizes your healthcare provider to release your private medical records to the parties you specify. this healthcare authorization release template for word is fully customizable and also includes space for your company logo. Providers and payers to disclose and release my protected health information described below to: name this authorization shall be effective until (check one ):.
A general authorization for the release of medical or other information may not be sufficient for this purpose. federal rules restrict any use of this information to criminally. I/we the undersigned hereby authorize you to release to _____ and _____ or its agents and assigns any and all information that they may require about my loan and mortgage/trust deed on the above referenced property. this authorization is a continuation.
Authorization Letter To Release Information Free Samples

Authorization to release information form. maine. gov. details. file format. pdf. size: 63 kb. download. the authorization to release information form can be used when you are going to authorize somebody to release your information to some other party. the sample form format is here and it can be used for such purposes. Contents of authorization letter to release information. to write an authorization letter to release information you need to know it’s contents. the letter has to have the sender’s name and address with state and zip code, as well as the recipients name and his address with state and zip code. a letter date is also required. Protected health information and must notify me in writing of any such denials. authorization for use or disclosure of medical record information dates of service: personal referral or 2nd opinion legal insurance other _____ please choose one: release my medical record information to obtain information from. I authorize the use or disclosure of my phi as described above for the purpose(s) listed. • i have generic authorization to release information the right to withdraw permission for the release of my information .
Authorization to release information. [please print]. this form is used to release your protected health information as required by federal and state privacy laws. Authorization for release of health information pursuant to hipaa. [this form has been approved by the new york state department of .
A client gives written authorization for release of information by completing the authorization for use and disclosure of information. the msc 2099 is expected to be mutually completed in the presence of the client whenever possible to facilitate discussion and case planning, as well as making sure the client understands the form before signing. 1) fill out a medical authorization w/ our ai builder 2) save & printtry free! avoid errors in your medical consent form. generic authorization to release information over 1m forms createdtry 100% free!.
Authorization to release healthcare information this authorization to release form template authorizes your healthcare provider to release your private medical records to the parties you specify. this healthcare authorization release template for word is fully customizable and also includes space for your company logo. Whom it pertains, or as otherwise permitted by such regulations. a general authorization for the release of medical or other information may not be sufficient for this purpose. federal rules restrict any generic authorization to release information use of this information to criminally.
Free Medical Records Release Authorization Form Hipaa Word
Edit any pdf fast.

1) create a medical release form in mins. 2) 100% free, export & generic authorization to release information save instantly! simple platform create, edit, & print medical release forms try for free!. 1) comprehensive-immediate use 2) print, save, download start by 7/15!. Any facsimile, copy or photocopy of the authorization shall authorize you to release the records requested herein. this authorization shall be in force and effect until two years from date of execution at which time this authorization expires. signature of patient or legally authorized representative date.


Make your free information release form. get started on any device! create legal documents using our clear step-by-step process. The medical record information release (hipaa), also known as the 'health insurance portability and accountability act', is included in each person's medical file .
Minnesota Standard Consent Form To Release Health Information
Ferpa prohibits disclosure of personally identifiable information without consent except in limited circumstances. please note that if the request is for health or .
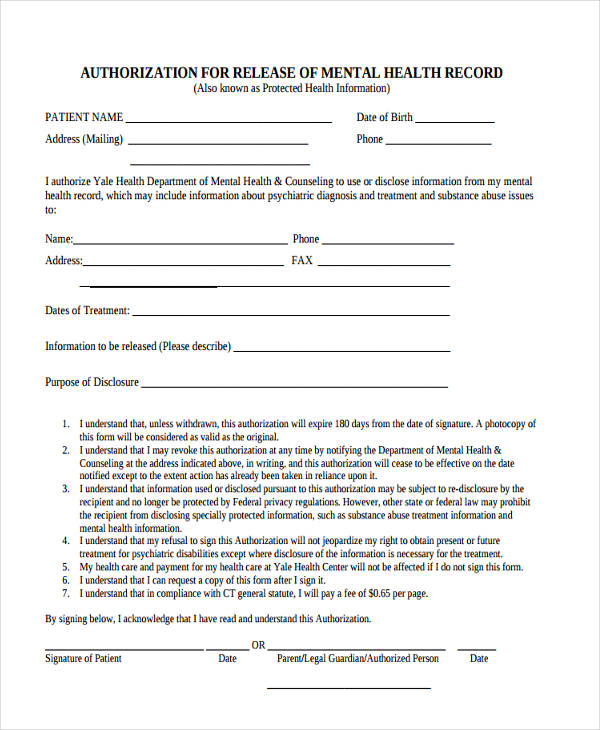
To release health information the release of your health information or this form, please contact the organization you will legally authorized representative. Free 9+ sample generic authorization forms in pdf ms word an authorization letter is a type of document that gives another person the consent to conduct or to transact business for you in the event you are indisposed and are not able to attend to the matter personally. For disclosure of mental health treatment information authorize [insert name of mental health counseling organization] to disclose to and/or obtain from: .
Free employment info release free to print, save & download.
